The Myth of Average: Time for Change
AiArthritis Voices 360 Main, Full Episode 72
Air Date: April 3, 2022
Join Tiffany and Deb, both persons living with AiArthritis diseases, then Tiffany and John O'Brien, CEO of the National Pharmaceuticals Council, as they put the topic of importance of innovation & treatment access in research and public policy 'on the table'. Learn how YOU can join efforts to impact change!
In this two segment episode, first join AiArthritis team - Tiffany and Deb - as they put a new show topic "on the table" for the first time: the importance of innovation in research and patient access to the treatments that are best for their individual characteristics. In this episode we introduce questions, like "Why does a treatment work for you and not me?" and "What if we don't tick all the boxes (are 'atypical', including having comorbidities) - how can I still access the best treatment for my unique needs?" The bottom line is that AiArthritis diseases are unique to the individual, and as a result, we may be better off using treatments that are not the same ones our health systems tell us we need to use. For change to happen, we need to hear stories from many patients (not just a few), but there are several barriers to achieving this. However, AiArthritis is working on a solution that involves creative, patient-led public policy classes focusing on four topics - two which are discussed today (innovation in research and value assessments). Listen to Deb and Tiffany explain more!
In the second segment, Tiffany welcomes John to the table, as his organization - the National Pharmaceutical Council (NPC) - published a few of the reports AiArthritis is referencing in our courses. Together they explore how new research can lead to improved patient care and potential access to the right treatment for individualized need and based on patient-doctor decided management. Finally, they start the conversation about value assessments (a complex and difficult process of assigning value and cost to medications), highlighting both an understood need for healthcare systems to provide fair access to all, while considering patient uniqueness and the future of personalized and precision medicine.

LISTEN TO THE FULL EPISODE THEN BE SURE TO TAKE A SEAT AT THE TABLE BY JOINING THE CONVERSATION!
(Scroll down the page to learn how!)
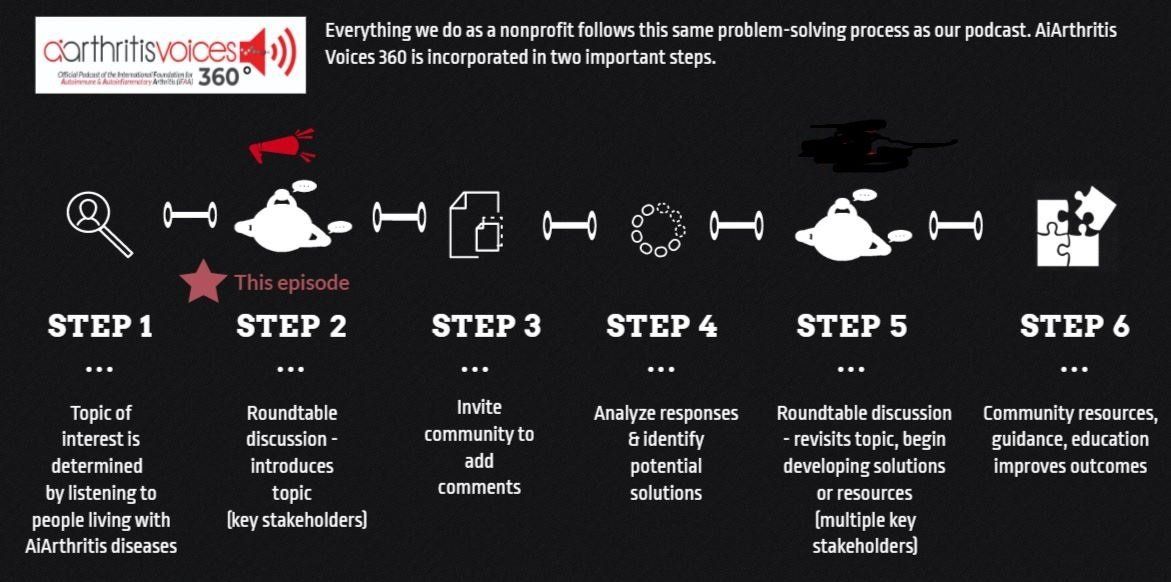
All our main 1st Sunday of the month episodes are either an initial "put the topic on the table" episode (Step 2 in our organization's 6-step problem solving process) or a "revisit to the table" episode, where we build on a past show because we have moved forward in developing help, tools, or projects around the issue (Step 5 in our organization's 6-step process).
After each show airs we spin off the conversation into many discussions over various formats, which we now call #360its (new in 2022)!

Show Notes:
Part One: Tiffany and Deb talk about the importance of innovative research and getting more patient voices involved in public policy (both which influence access to therapeutic care).
:53: Tiffany introduces show, herself (nr Axial Spondyloarthritis), and co-host Deb introduces herself (Rheumatoid Arthritis and several comorbidities)
- 2:25: Tiffany explains the topic of the show today, which involves patients who are not typical, including those with many diagnoses or who do not “check the boxes”.
- 3:35: Today we will focus on the importance of being “average” and “not-so-average”. The time being now for all of us to come forward and speak out in regards to our access to therapies and disease management - through public policy and research efforts. This is especially important for those who don’t tick the boxes, or a model, textbook perfect patient.
- 4:25: Tiffany mentions the second half of the show will feature a guest, John O’Brien, President & CEO of the National Pharmaceutical Council (NPC) who will be discussing their paper, “The Myth of Average”, and the importance of innovation in research and understanding value assessments (or the processes around health systems procedures that help determine which medications we are able to access).
- This is a problem when we don’t all fit a ‘general patient population’ when we are thinking about policies that are centered around access for the average - and in a time when we are moving towards a world of precision medicine (treating the individual).
- How can patients come to the table and make a difference so we don’t lose access to options?
- 5:25: Tiffany and Deb discuss their patient journeys and, specifically, how they would not be considered ‘typical’, or classified in the group of general patient population. “We are all unique.”
- Tiffany further explains how her current diagnosis did not exist a decade ago, so thankfully for research her disease now has a name and treatments that work well for her.
- 8:45: Deb and Tiffany discuss how different therapies work for different people, which is important to understand. “What works for you may not work for me.”
- 9:27: Tiffany asks listeners to think about the evolution of our patient journeys and, as a result, the importance of patients/supporters to stay connected with their legislators (people partially responsible for access to healthcare) over time so they can see that our diseases are not static. They often evolve and, in turn, our treatment needs can change.
- 11:40: Tiffany and Deb discuss the analogy of using cough medicine. Why is “your” cough medicine better? We need to realize drugs in the same classes work differently because they have various differences that, in turn, react differently in each person’s body. “This is why AiArthritis is highly invested in precision medicine, or matching the right person to the right treatment at the right time.”
- We are also invested in personalized medicine, or personal preferences, which also factor in.
- 13:18: Tiffany states the organization's mission to help others, like them, have a voice - alongside other stakeholders as equals - so, together, we can solve problems that impact education, advocacy (public policy), and research.
- 13:45: Tiffany explains the role of ethics in healthcare access, referencing a paper she authored in 2015, the Ethics of Step Therapy, in collaboration with two bioethicists and “bestie” Kathleen Arntsen from Lupus and Allied Diseases, Inc., where AiArthritis learned all about the different roles of ethics for both health providers and doctors. She specifically explains the ethical Principle of Justice, which involves the responsibility to ration healthcare for all. “If we are going to change, we need to meet in the middle, respectful of the agencies who need to consider access for all.
- 15:50: They discuss show design, in that this is the first time this topic was put ‘on the table’. In 2022, we are starting “360its”, or spin off episodes and segments that will be in a variety of methods and platforms so all people can contribute to this conversation (globally). Then, together, we can all be part of the solution in regards to healthcare access and desire for innovation to continue.
- Keep in mind, perspectives may vary depending on where you live. For example, in socialist societies, value assessments - which tend to favor general patient populations - may be more accepted.
- 17:05: They discuss research and ‘atypical’ factors into this. Cost savings is often based on citing credible research, which is mostly conducted in general patient populations (or whomever signs up to participate!)
- 17:50: Patient stories are vital to helping legislators humanize health access issues, but it’s always a challenge finding stories - or the stories are from the same people. So AiArthritis spent 2021 figuring out why and, as a result, identified several barriers to participation, including lack of clarity and confidence.
- As a result, AiArthritis is launching a patient-led creative classroom program in 2022 that will cover four topics, including innovation and value assessments. Goals: 1) Increase number of patients/supporter voices in public policy and story sharing (including demographic contribution), 2) Recruit our own organization ambassadors, 3) Build confidence, 4) Identify the issue in relationship to self and others (patient to patient invitation to learn how to have a voice).
- 30:10: They discuss how this conversation will 360it and how to get involved in this new program: https://www.aiarthritis.org/advocacy
- 30:55: Part of the program will involve a program library of resources, including featuring The Myth of Average publication by the National Pharmaceutical Council (NPC)- which is why we are talking to John from the NPC next.
- 30:23: Tiffany thanks Deb
Part Two: Tiffany and John discuss innovation in research and value assessments (measurements used, in some cases, to determine patient access to certain treatments)
- 31:39: Tiffany welcomes John to the show, who introduces himself and the NPC
- 32:58: Tiffany explains John is ‘at the table’ because AiArthritis, who has developed a new patient-led public policy education program, is referencing several of the NPC’s publications for the class library (including the Myth of Average). The piece is in keeping with AiArthritis’ core priorities to help foster precision medicine and assess the right treatments for the individual.
- 35:42 John explains that innovation means the never ending search for cures and new treatments and why this resonates with him.
- Why does one treatment work for one person and not the other?
- Uses the example of Tiffany’s journey, as she was diagnosed in 2009 before her disease had a name (nr-axial spondyloarthritis). So researchers were finding solutions for people like Tiffany, the Mystery Patient, and that’s innovation.
- “This is all why it is essential that patients and researchers stay connected during the development process.”
- 39:00: Patients who are atypical, but who are lumped into the general patient population model, may risk being on the wrong treatment and that can have negative consequences. “Putting me on the right treatment that was indicated for my disease made a world of difference. It was like night and day.”
- 40:07: Tiffany tells us a story about her quality of life challenges prior to access to the right treatment, which involved the inability to get out of bed in the morning.
- 40:53: Also, people like Deb - who have exhausted all treatments - what do these patients do? Patients like us need to understanding the importance of research and the public policies that can influence our access to the treatments best for our individual needs. Join AiArthritis’ efforts at https://www.aiarthritis.org/advocacy
- 42:15: John talks about the importance of the patient-doctor decision for treatments, which can be sidetracked if the healthcare system does not cover that therapy.
- Researchers ask, “Why do different individuals have different responses to the same treatments?”
- Furthermore, if the treatment was designed for the general patient population, how will this impact a patient’s access to their doctor recommended therapy?
- The Myth of Average report highlights that age, genetics, ethnicity, behaviors, biology, and other individualized factors are not always considered when rationing treatments on a population level. “Patients should have access to the treatment that their doctor believes is clinically relevant for them.”
- 48:00: Tiffany talks in detail about AiArthritis’ Ethic of Step Therapy investigation (2015) - which has relevant takeaways regardless of health system (location): patient-centeredness, fairness, clinical relevance.
- They revisit the Principle of Justice (from Part One with Deb)
- The ah-ha moment that led to the conclusion of the paper was a result of Tiffany’s inability to be included in clinical trials because she was an atypical patient. She realized that clinical trials include patients who meet a general patient population criteria - the same research that insurance companies cite to justify their cost savings. However, in cases like Tiffany - where the patient is atypical - then the decision should default to the doctor, who is ethically obligated to treat to the individual characteristics of the patient. “Drop mic.”
- 50:44: This ethics paper led to the research work - and public policy work - we do at AiArthritis, in part, because a lot of money goes into this research using the general patient population, yet only 40-60% will respond once that drug goes to market (because the rest of us are atypical). “We need more treatments” for the rest of us.
- Shout out to Autoimmune Association and the Let My Doctor’s Decide Initiative, which AiArthritis serves as an advisor.
- 52:02: John tells a story about how patients/supporters often understand the mechanisms of their disease and the different treatments researchers as well as the company themselves. “So not just at this table, but we have so much to learn from each other - especially when it comes to what the condition is like in the real world.”
- 53:25: John talks about health technology assessments (value assessments), what they are - including some access barriers they may cause (due to lack of transparency, caregiver burden, and drug measurement vs personalized experiences).
- Provides an example of employer based insurance (USA) if an employee is unable to work due to inability to access the best treatment for them.
- 55:42: John defines health technology assessments (HTAs), including the history of them and further discusses Quality Adjusted Life Years (QALYs) - which in his opinion can be discriminatory for people living with disabilities.
- 1:00:08: There is a need to cut costs and have a well distributed system of rationing spending. Even on some HTA websites in their own explanation of how these work they state the process is not designed for the individual but rather for the population. However, in a world that’s moving towards precision medicine, and considering the patients who have exhausted all treatments, how do we ensure value assessments can be fair and considerate of the new science?
- They further discuss the QALY.
- No one is telling employers who are choosing health plans (USA) that if their employee isn’t able to work because they don’t have access to the right treatment that it could end up costing them more in time off, hospitalizations, and overall less work production.
- “This is the risk of using QALY’s when trying to establish population based coverage decisions.”
- Tiffany confirms that it’s difficult to work if you have brain fog, pain, or fatigue.
- 1:03:35: Tiffany reminds the audience that now in 2022 we are spinning off from each episode - any bullet point, any topic segment - and continuing the conversation in a variety of ways so we can include all of you in the conversation. Called #360its. Patients, supporters, legislators, researchers, pharma, etc - we need you all at the table!
- “The people who I always learned the most from are the patients.” Patients need to share their experiences.
- 1:06:00: Tiffany mentions a good 360it would be to discuss the continued need to use shared decision making in healthcare (patient-doctor decisions), because that is also relevant in regards to accessing the treatment that may be innovative and new (if that is the right treatment for us). Personalized and precision medicine consideration.
- 1:07:20: The research the NPC does is to help patients gain access to medications and foster innovation. “What If Groundbreaking Medicines Never Existed?” paper, which outlines where we would be today without drug innovation. Tiffany suggests that people read this, then let’s do a 360it to discuss.
- 1:09:15: Tiffany reiterates the reason John is here is because the work the NPC does is in line with our AiArthritis work to fight for precision medicine (access to the right treatments at the right time for the individual person's needs). As such, we are including a few of their reports in our resource library in our new patient-led public policy education program. Learn more and sign up at https://www.aiarthritis.org/advocacy.
- 1:10:10: Tiffany thanks John for pulling up a seat at the table.
- 1:10:31: Tiffany closes out the show. If you like the show and listen on your favorite podcast station, please subscribe and give us a rating.
- Find all the episodes at our website at www.aiarthritis.org/talkshow
- Also, if you want to help us continue offering this program, please consider a donation, because your support makes this show possible!
- Find us on all social media channels at @IFAiArthritis where you can message us to have a seat at the table or email us at podcast@aiarthritis.org.
360its!
After this initial topic of public policy and access to therapies was 'put on the table' for the first time in April 2022, we opened the topic up for others to start weighing in. This is called a #360it. 360it's can spin off into any direction, so the conversation continues and more voices are included in any solutions we work on.
#360it Spin Off Issue: Medicare/Medicaid USA - Hosted by Patrice (Rheumatoid Arthritis) and Rick (Ankylosing Spondyloarthritis, Rheumatoid Arthritis)
What challenges do YOU have if you are on Medicare/Medicaid? Did you know there are efforts underway to reform these services? Your input matters! Tell us what problems you deal with when it comes to Medicare/Medicaid:
- Click HERE to submit using our RANT submission form (can be anonymous).
- Add your comments to the YouTube video feed.
Stay tuned... more 360it's coming your way!
In the meantime, ANY issues you have with accessing your therapies (pharma or non-pharma), falls under this category, because legislation and government often regulate this. Submit your issues today using our RANT page. Who knows - it may become the next 360it!
Pull up your seat at the table
Now it's YOUR TURN to join the conversation!


What do you think about this episode?
We want to know what you think! By continuing the conversation with your opinions and perspectives - we all get a better understanding of the problems facing our community. Better yet, through these conversations we can start working and developing solutions.
We mean it when say 360. Not only do we want your input anytime and anywhere, but we also are eager to see where the conversation will take us. So please, "pull up a seat at the table" and let's start talking!
Email us at podcast@aiarthritis.org, message us on social media (find us by searching for @IFAiArthritis)
Continue the conversation in our own AiArthritis Voices 360 Talk Show Group!
Pull up a seat and join the conversation on the topic from today and past episodes. You may even get an opportunity to talk directly with the co-hosts and any episode guests!
The
AiArthritis Voices Program
Our AiArthritis Voices 360 Talk Show is just a piece of larger program - the AiArthritis Voices Program.
AiArthritis Voices is our program where people living with AiArthritis diseases and other stakeholders who we need 'at the table' to solve problems that impact education, advocacy, and research sign up to have a voice in our initiatives.
If you want to get more involved, and see more of the opportunities we have for you (and all stakeholders) please check out the
AiArthritis Voices Program. Unite with others around the world to talk, learn, and connect.
Your Co-Hosts & Guests: Who is at the table this episode?

Tiffany Westrich-Robertson
Tiffany is the CEO at International Foundation for AiArthritis and uses her professional expertise in mind-mapping and problem solving to help others, like her, who live with AiArthritis diseases work in unison to identify and solve unresolved community issues. For the last several years, she has continued her education in research, including becoming a professional focus group moderator, and translated this experience at our organization to develop award-winning, innovative projects that are taking patient engagement to next levels.
Tiffany has served on several advisory boards, including those to advance patient voices in policy, clinical trials, and precision medicine. In addition to reviewing grants at PCORI and for the Department of Defense, she was the sole patient grant reviewer for the National Institute of Arthritis and Musculoskeletal and Skin diseases from 2015-2018. She currently participates as a Patient Research Partner for OMERACT (Outcome Measures in Rheumatology), co-leads our organizations' international effort to advance patient voices in rheumatology research (the ACTion Council) and has dedicated her professional career to developing other patients to utilize their voices to impact the future of millions.
- Facebook: @tiffanyAiArthritis
- Twitter: @tiffwrobertson
- LinkedIn: @tiffanywestrichrobertson

Deb Constien
I live in Sun Prairie, just outside Madison Wisconsin, with my husband Tim of 28 years and 23year old son Jacob. I was diagnosed with Rheumatoid Arthritis at the young age of 13. I am a medically retired Registered Dietitian, graduating college with majors in Dietetics and Biology. I have been a volunteer and representative for AiArthritis for the past 7 1/2 years and really enjoy using my scientific expertise to help in the patient journey. In addition to volunteering for AiArthritis, I also volunteer for the Arthritis Foundation, the Advisory Council for WREN- Wisconsin Research Education Network, Patient Family Advisor- PFA on an International PCORI research study for ACP- Advanced Care Planning. I am also on an OMERACT study group for Shared Decision Making.
- Facebook: @deb.majcherconstien
- Instagram: @debconstien
- Twitter: @debconstien
- LinkedIn: linkedin.com/in/deb-majcher-constien-59945429
- YouTube: debconstien
- TikTok: debconstien

John M. O'Brien
John M. O'Brien, PharmD, MPH, is the president and chief executive officer of the National Pharmaceutical Council (NPC), which sponsors and participates in research on the appropriate use of pharmaceuticals and the clinical and economic value of pharmaceutical innovation. Dr. O’Brien’s broad experience spans the private sector, academia and government. Prior to NPC, Dr. O’Brien was senior advisor to the U.S. Secretary of Health and Human Services and deputy assistant secretary of planning and evaluation (health policy). He also has held senior policy positions in the life sciences and managed care industries, including at CareFirst BlueCross BlueShield and the Centers for Medicare & Medicaid Services (CMS), and served as a health policy fellow in the U.S. Senate. Dr. O’Brien earned his doctorate in pharmacy at Nova Southeastern University and his master’s degree in public health at the Johns Hopkins Bloomberg School of Public Health.
- Twitter: @drjmob
- LinkedIn: @drjmob


Love the show? Help us make sure we stay on the air by making a donation.
Your contribution helps us continue the work we do every day to improve the lives of millions worldwide.
Sign up for our newsletters
International Foundation for AiArthritis
6605 Nottingham Ave.
St. Louis, MO 63109-2661
Toll Free: 1-877-609-4226
Text: 1-314-282-7214
Copyright 2024. All rights reserved. Information on this site is intended for informational purposes only Our foundation does not engage in the practice of medicine. Please consult a physician to obtain personal healthcare and treatment options. 501(c) 3 Nonprofit Tax ID: 27-1214308.